Summary
- Company: MIM Software
- In Collaboration With: Product, Engineering, Clinical Science, Site Development, and Sales
- Tools: Figma and Google Suite
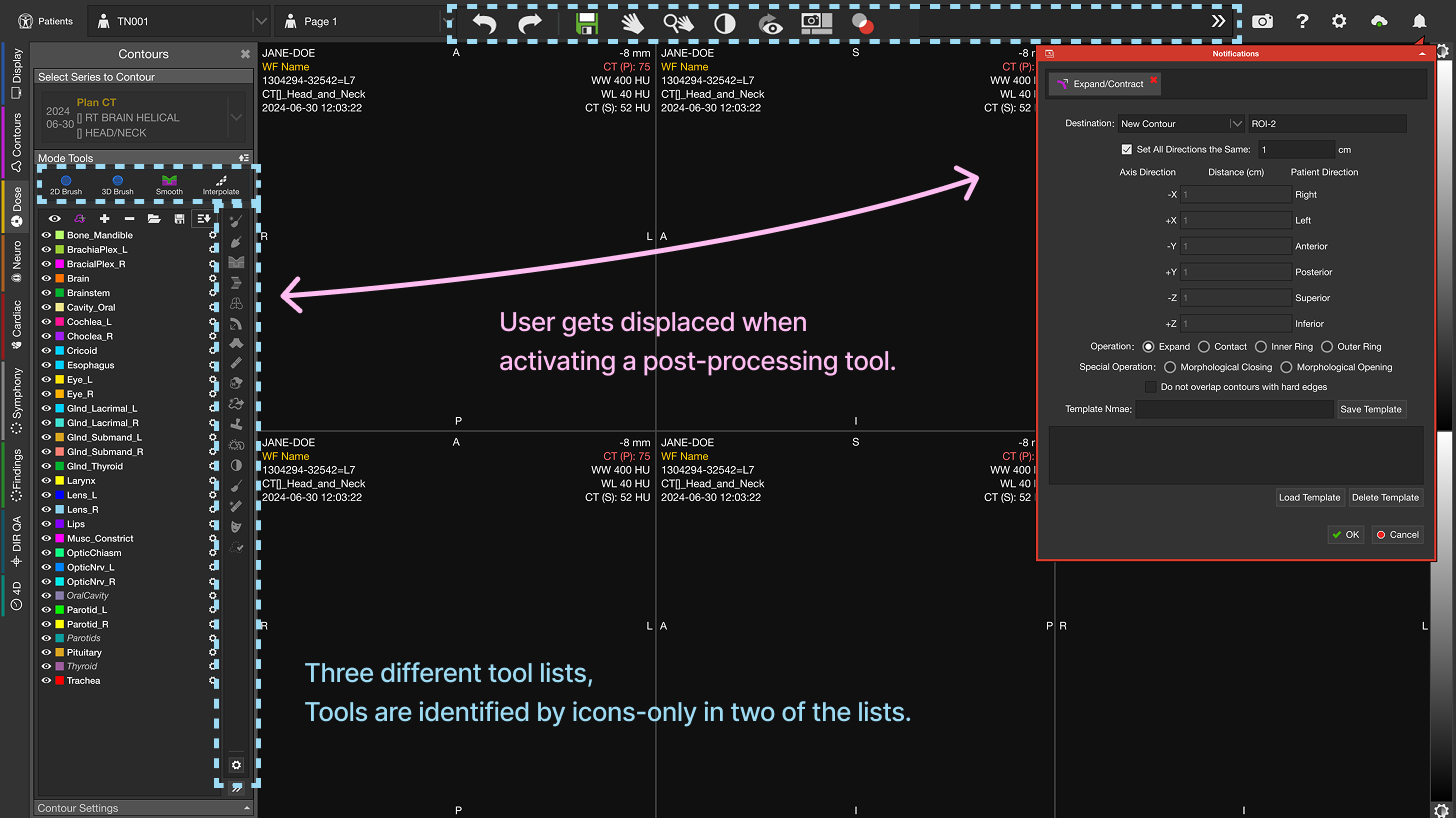
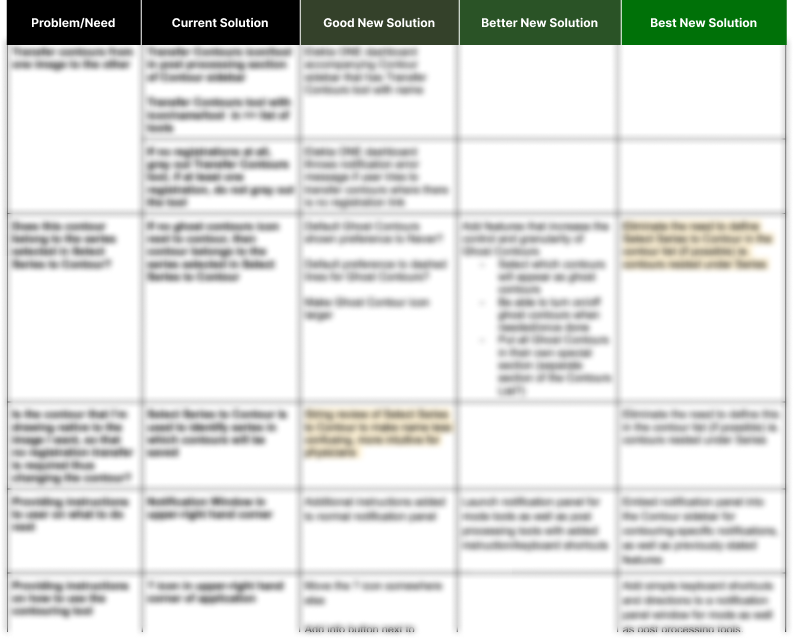
- The Problem: We believed the complexity of our contouring tools was becoming a barrier for MIM adoption amongst physicians.
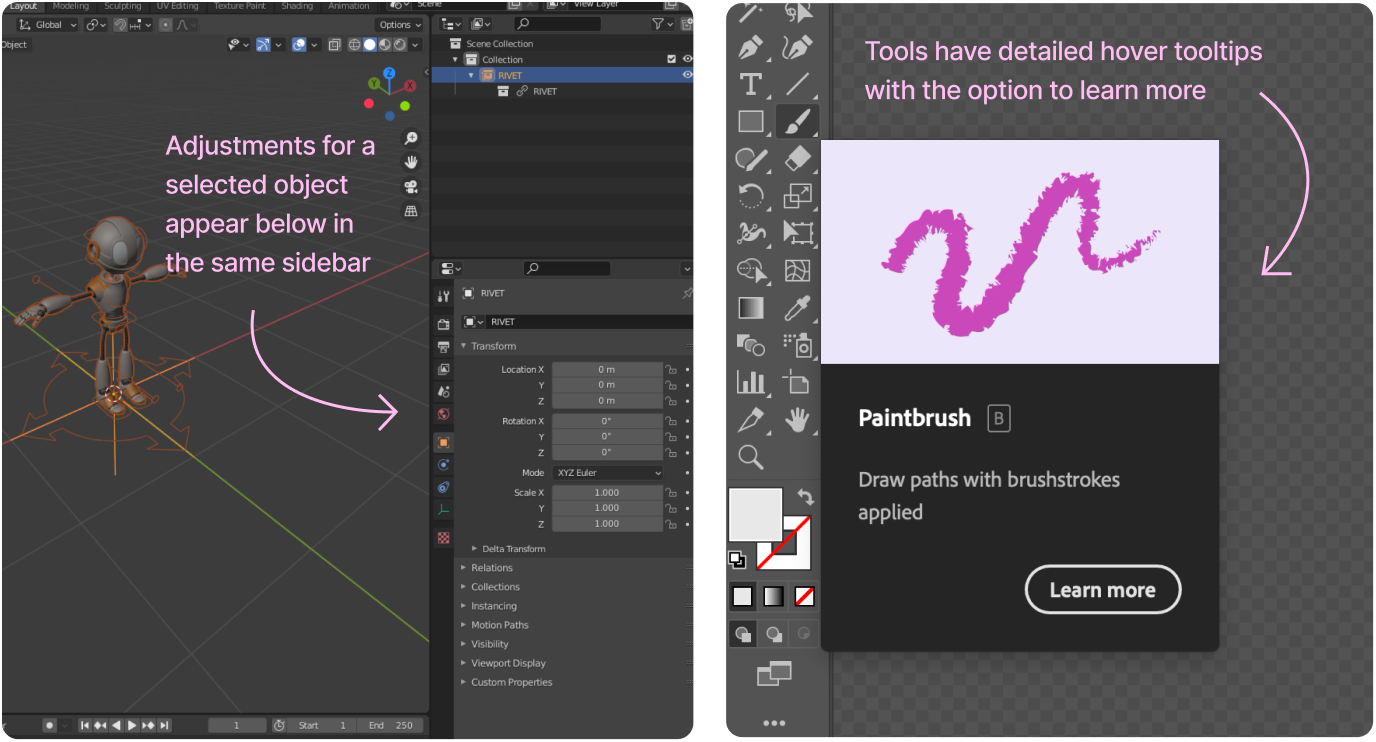
- The Goal: Improve contouring accessibility for physicians, making it easier to learn and find the tools needed for daily work.